Fetal Hydronephrosis
Fetal hydronephrosis is a common condition in which excess fluid is detected in a baby’s kidney due to a buildup of urine. This can occur when the baby is still in the mother’s uterus. As many as 1 in 100 pregnancies in the United States have some evidence of fetal hydronephrosis.
About Fetal Hydronephrosis
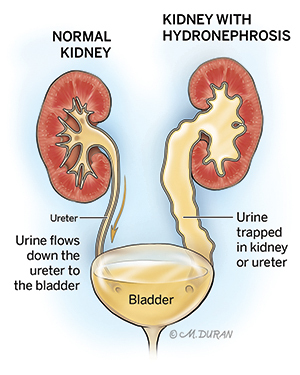
Urine that is made in the kidneys normally drains out of the kidneys completely, traveling down through the ureter (the tube that connects the kidneys to the bladder) and into the bladder, where the urine is emptied out of the body. Hydronephrosis is a treatable condition in which urine gets trapped in one or both kidneys, most commonly as a result of a blockage, causing the urine to drain slower than it should. Hydronephrosis can occur in people of all ages.
Fetal hydronephrosis is often detected when the kidney appears swollen on a fetal ultrasound. When a small amount of fluid is observed in the center of the kidney (the renal pelvis) during a fetal ultrasound, this is known as pyelectasis. A larger amount of fluid observed in the renal pelvis is known as hydronephrosis. When a blockage has occurred below the level of the kidney, the ureter can become enlarged and appear “sausage-like,” which is known as hydroureter.
There are different degrees of fetal hydronephrosis, ranging from grade 1 (most mild) to grade 4 (most severe). The grading system is based on how dilated the renal pelvis and the calyces (chambers of the kidney through which urine passes) are as well as the amount of renal parenchyma (the functional tissue within the kidney that filters blood to remove waste) that is present. The more severe grades of hydronephrosis are often associated with problems that develop later in life.
Symptoms of Hydronephrosis
Infants with hydronephrosis usually do not have any symptoms. If a child has more severe hydronephrosis, they may show symptoms.
Symptoms of hydronephrosis may include:
- Abdominal pain with nausea and/or vomiting, especially after large fluid intakes
- Flank pain (pain above the hipbone, slightly to the back)
- Hematuria (blood in urine)
- Urinary tract infections
Causes of Fetal Hydronephrosis
The most common causes of fetal hydronephrosis are obstructions (blockages) that restrict urine from flowing through the kidney and into the bladder.
Types of fetal hydronephrosis obstructions include:
- Ureteropelvic junction (UPJ) obstruction is a blockage at the point where the kidney meets the ureter.
- Ureterovesical junction (UVJ) obstruction is a blockage at the point where the ureter meets the bladder.
- Posterior urethral valves (PUV) are obstructive membranes (pieces of tissues) that develop in the lower urethra (the tube in the penis) in males prior to birth.
- Ureterocele occurs when swelling in the ureter causes the ureter to balloon at its opening into the bladder, forming a sac-like pouch.
Other causes of fetal hydronephrosis may include:
- Vesicoureteral reflux occurs when urine in the bladder flows back up the ureters and often back into the kidneys.
- Ectopic ureter occurs when the ureter does not connect properly to the bladder, causing the ureter to drain urine somewhere outside the bladder.
- Neurogenic bladder is a condition in which the nerves that carry messages from the bladder to the brain and from the brain to the muscles of the bladder do not work properly.
Complications Associated With Fetal Hydronephrosis
Fetal hydronephrosis is not associated with any health risks for the pregnant mother. In approximately 50% of cases, fetal hydronephrosis resolves by the third trimester. If fetal hydronephrosis gets worse as pregnancy continues, it usually does not cause any serious problems in the baby and an early delivery is not necessary. If your baby has a more severe case of fetal hydronephrosis, in utero treatment and treatment after birth may be needed, which may include surgery to help resolve the issue and prevent long-term kidney problems.
Diagnosing Fetal Hydronephrosis
Fetal hydronephrosis is typically diagnosed during a routine fetal ultrasound at around 20 weeks (5 months) of gestation. If during this ultrasound only pyelectasis is detected, fluid measurement is monitored throughout the remainder of the pregnancy. If the fluid in the renal pelvis reaches 10 millimeters or more, hydronephrosis is diagnosed.
Pregnancy With Fetal Hydronephrosis
After the initial evaluation, you will be scheduled for ultrasounds every 3 to 4 weeks to monitor the hydronephrosis. During your pregnancy, you may be referred to meet with a pediatric urologist who can assist in the care for your baby if surgery is needed to fix the hydronephrosis after birth. You may also be scheduled to meet with a pediatric nephrologist, a specialist who treats kidney damage.
You are able to go into spontaneous labor and having a vaginal delivery near your due date is safe for a baby with hydronephrosis.
Treating Fetal Hydronephrosis
Treatment of fetal hydronephrosis is needed if there is a severe blockage in the urethra known as lower urinary tract obstruction (LUTO). In a male fetus, this is usually caused by posterior urethral valves (PUV) that have blocked the urine flow from the bladder to the penis. In severe cases, the urine is completely blocked and the bladder becomes quite large. The urine can then back up into the ureters and into the kidneys, causing hydroureters and hydronephrosis. The blockage can also cause there to be an absence of amniotic fluid around your baby, a condition known an anhydramnios, which can lead to poor development of the baby’s lungs (pulmonary hypoplasia) and severe problems with breathing soon after birth.
If your baby has a lower urinary tract obstruction with no amniotic fluid, a bladder shunt (thin tube) may be placed, using a special needle that is inserted into the bladder, to allow it to drain outside of the fetus. This can be done while the fetus is still in the womb. Although a bladder shunt can allow urine to flow again, it often does not reverse the damage to the kidneys that has already occurred. Placement of a bladder shunt can, however, result in a normal amount of amniotic fluid around the fetus and improved breathing after birth.
Evaluation After Birth
After birth, your baby will likely undergo an ultrasound to examine at the kidneys. Your pediatric urologist may also recommend that your baby receive antibiotics to prevent infection in the kidneys if they are experiencing urinary reflux in which the urine flows backward from the bladder when your baby pees.
When your baby is several weeks old, you may be scheduled to bring your baby to the hospital to undergo a special test known as a voiding cystourethrogram (VCUG). During this test, a catheter (small tube) will be placed through the baby’s urethra and into their bladder. A special dye is injected through the catheter, filling the baby’s bladder. When the bladder gets full, the baby will pee on their own and a special X-ray will be completed to determine if any of the dye is moving backward toward the kidneys. In many cases, the hydronephrosis can be monitored and is expected to improve. In more severe cases, surgery may be required to correct the blockage to prevent long-term kidney problems.
Care Team Approach
The Comprehensive Fetal Care Center, a clinical partnership between Dell Children's Medical Center and UT Health Austin, takes a multidisciplinary approach to your child’s care. This means you and your child will benefit from the expertise of multiple specialists across a variety of disciplines. Your care team will include fetal medicine specialists, obstetricians, neonatologists, sonographers, palliative care providers, fetal center advanced practice providers, fetal center nurse coordinators, genetic counselors, and more, who work together to provide unparalleled care for patients every step of the way. We collaborate with our colleagues at The University of Texas at Austin and the Dell Medical School to utilize the latest research, diagnostic, and treatment techniques, allowing us to identify new therapies to improve treatment outcomes. We are committed to communicating and coordinating your care with your other healthcare providers to ensure that we are providing you with comprehensive, whole-person care.
Learn More About Your Care Team

Comprehensive Fetal Care Center
Dell Children's Specialty Pavilion
4910 Mueller Blvd. Austin, TX 78723
1-512-324-0040
Get Directions