Multicystic Dysplastic Kidney
Multicystic dysplastic kidney (MCDK) is an abnormal fetal development of one or both, although rare, kidneys in which the kidney consists of multiple irregular fluid-filled cysts. Multicystic dysplastic kidney occurs in approximately 1 out of every 2,400 live births in the United States.
About Multicystic Dysplastic Kidney
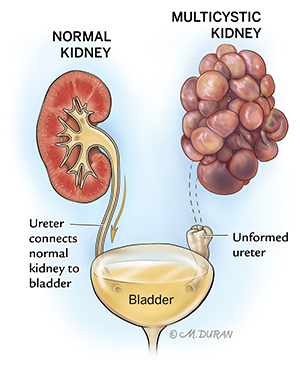
At around 5 weeks of gestation, the bud of the tissue that forms the ureter (the tube that connects the kidney to the bladder) connects to the tissue that will later form the kidney. If this process fails to occur properly, a kidney consisting of multiple irregular cysts (sac-like pockets that contain fluid) occurs. This is known as a multicystic dysplastic kidney. Due to the lack of connection to the bladder, this kidney cannot produce normal urine. Fortunately, if only one kidney is affected (unilateral), the remaining kidney is typically able to take over the kidney function in the baby. If both kidneys are affected (bilateral), the baby will likely not survive. A unilateral multicystic dysplastic kidney is twice as common as a bilateral multicystic dysplastic kidneys.
Symptoms of Multicystic Dysplastic Kidney
A multicystic dysplastic kidney does not cause any symptoms.
Causes of Multicystic Dysplastic Kidney
Although rare, the occurrence of a multicystic dysplastic kidney can run in families due to a genetic trait; however, the majority of cases occur as an isolated event. Some studies suggest certain viral infections and some drugs may also play a role in the development of a multicystic dysplastic kidney if exposure occurs during a critical stage of fetal development.
Complications Associated With Multicystic Dysplastic Kidney
The occurrence of a multicystic dysplastic kidney is rarely associated with any health risks for the pregnant mother. The main concern associated with a multicystic dysplastic kidney is related to the condition of the contralateral kidney (the kidney opposite of the affected kidney). If this kidney remains unaffected, without blockage to urine, the fetus should not develop any problems. In approximately 10% of cases, the multicystic dysplastic kidney decreases in size as the pregnancy progresses. In another 10%, it can increase in size. If the cysts grow in size, your doctors may become concerned about the size of the baby’s belly and whether the baby will fit through the birth canal if delivered vaginally. If both kidneys are multicystic, then there is no fetal urine production (which contributes to the amount of amniotic fluid) and the amniotic fluid around the fetus will being to disappear at around 16 weeks (4 months) of gestation. If this is the case, the fetal lungs will not develop (pulmonary hypoplasia) and the chance for newborn survival is minimal. In approximately 5% of cases, chromosomal abnormalities occur in fetuses with a multicystic dysplastic kidney.
Diagnosing Multicystic Dysplastic Kidney
A multicystic dysplastic kidney is typically diagnosed during a routine fetal ultrasound at around 20 weeks (5 months) of gestation. It appears as multiple dark fluid-filled cysts that essentially replace the entire kidney.
Pregnancy With Multicystic Dysplastic Kidney
After an initial ultrasound evaluation, you will likely be scheduled for ultrasounds every 3 to 4 weeks to monitor your baby’s rate of growth, the growth of the multicystic dysplastic kidney, and the status of the other kidney. In some cases, you will be scheduled to meet with a genetic counselor to discuss your baby’s risk for developing chromosomal problems as well as the available tests that can be completed during your pregnancy to identify these types of problems. During your pregnancy, you may also be referred to meet with a pediatric urologist who can assist with any potential kidney problems your baby may have after birth.
A vaginal delivery is usually safe for babies with a multicystic dysplastic kidney. Most women with a baby in utero with a multicystic dysplastic kidney will be allowed to go into spontaneous labor near their due date. In some cases, delivery by C-section may be necessary if the kidney grows very large in size, causing concern for the safety of the fetus during vaginal delivery.
Treating Multicystic Dysplastic Kidney
There are currently no forms of fetal surgery available for treating multicystic dysplastic kidney. In nearly half of cases, the multicystic dysplastic kidney will decrease in size on its own. If the multicystic kidney is very large at birth and causing problems with the baby’s breathing or eating, a decision may be made to do surgery and remove the kidney. Most babies with a multicystic dysplastic kidney do not experience long-term problems as long as their unaffected kidney remains normal. If the multicystic dysplastic kidney gets larger or your baby develops high blood pressure, your pediatric urologist may decide to perform surgery to remove the affected kidney.
Evaluation After Birth
After birth, unless unusual problems arise, your baby will be transported to the normal nursery or be allowed to remain in the room with you. Your baby will likely undergo an ultrasound of the kidneys. If there is evidence of extra fluid in the unaffected kidney, your pediatric urologist may recommend that the baby receive antibiotics once the baby is discharged. This is to prevent infection in the normal kidney in the case that some of the urine is flowing backwards from the bladder when the baby pees (urinary reflux).
When your baby is several weeks old, you may be scheduled to bring your baby to the hospital to undergo a special test known as a voiding cystourethrogram (VCUG). During this test, a catheter (small tube) will be placed through the baby’s urethra and into their bladder. A special dye is injected through the catheter, filling the baby’s bladder. When the bladder gets full, the baby will pee on their own and a special X-ray will be completed to determine if any of the dye is moving backward toward the kidneys.
Care Team Approach
The Comprehensive Fetal Care Center, a clinical partnership between Dell Children's Medical Center and UT Health Austin, takes a multidisciplinary approach to your child’s care. This means you and your child will benefit from the expertise of multiple specialists across a variety of disciplines. Your care team will include fetal medicine specialists, obstetricians, neonatologists, sonographers, palliative care providers, fetal center advanced practice providers, fetal center nurse coordinators, genetic counselors, and more, who work together to provide unparalleled care for patients every step of the way. We collaborate with our colleagues at The University of Texas at Austin and the Dell Medical School to utilize the latest research, diagnostic, and treatment techniques, allowing us to identify new therapies to improve treatment outcomes. We are committed to communicating and coordinating your care with your other healthcare providers to ensure that we are providing you with comprehensive, whole-person care.
Learn More About Your Care Team

Comprehensive Fetal Care Center
Dell Children's Specialty Pavilion
4910 Mueller Blvd. Austin, TX 78723
1-512-324-0040
Get Directions